
Falls in elderly patients – a first aid guide
In this first aid blog post we discuss the first aid for falls in elderly patients. While less than ten per cent of falls result in  fractures, accidents are the fifth leading cause of death in the elderly, with falls constituting two-thirds of accidental deaths.
fractures, accidents are the fifth leading cause of death in the elderly, with falls constituting two-thirds of accidental deaths.
Although most falls do not result in serious injury, the other consequences, which are sometimes more serious and have devastating effects on the patients’ life, can include:
- psychological problems, for example, a fear of falling and loss of confidence in being able to move about safely. Between 40 and 70 per cent of elderly people who have fallen will restrict their daily activities because they are afraid that they will have another fall;
- loss of mobility, leading to social isolation and depression;
- increase in dependency and disability;
- hypothermia;
- pressure-related injury such as pressure sores. Approximately ten per cent of patients may remain on the ground for over 24 hours which can result in pressure sores, and deep vein thrombosis;
- infection.
Up to one third of people die within one year of their hip fracture and significant numbers of patients will suffer loss of independence due to reduced mobility.
Who is at risk?
Risk factors for falls and injuries can include:
- sensory impairment. Vision and hearing difficulties can increase the risk and number of falls;
- medical conditions and emergencies that affect balance or weakness, such as stroke and Parkinson’s disease;
- dementia, especially as it affects balance, judgement and problem-solving ability;
- musculoskeletal disorders, particularly those affecting the lower limbs, causing weakness or deformity;
- medications, especially those with sedative effects, such as sleeping tablets or anxiety medication. Cardiovascular drugs and anti-hypertensives can also result in falls by lowering blood pressure;
- depression, especially when the patient is using anti-depressant medication;
- use of alcohol, even in small doses, can affect balance and gait, increasing the risk of falls;
- increased age; the older the patient the greater the risk is of falls and injuries;
- poor energy absorbing capacity of tissues or bone, for example brittle bones are more easily fractured and paper thin skin and reduced fatty tissue can result in severe bleeding and damage to the tissues underneath.
Assessing a patient who has fallen
The key components of a fall history can be remembered using the acronym SPLATT.
- signs and symptoms;
- previous falls;
- location of fall;
- activity at time of fall;
- time of fall;
- trauma, both physical and psychological.
Investigating the cause of the fall is just as important as treating any injury sustained. Patients should be asked what they were doing and feeling at the time of the fall, especially whether it was a mechanical fall or due to dizziness or other symptom.
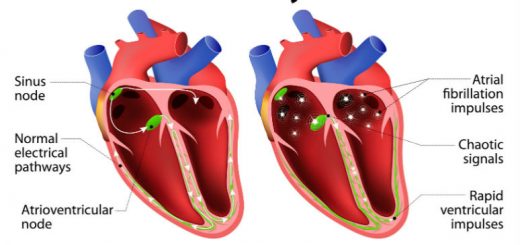
A myocardial infarction (heart attack), for example, may cause sufficient damage to the heart to decrease the blood flow to the brain resulting in syncope (fainting) or precipitate a cardiac arrhythmia (abnormal heart rhythm) which can also produce syn- cope (fainting).
When examining the patient also look for clues to the reason for the fall, such as previous medical conditions, medications, signs of mobility problems, for example a stick or walking frame, a smell of alcohol, a poorly lit environment or trip hazards such as mats.
As elderly patients are very prone to injury, even from minor trauma, ensure that a thorough examination to find all injuries, if time allows, is carried out.
One US study found that elderly patients presenting to a casualty department with one complaint from trauma were found to have a second injury they were not aware of.
Thorough assessments and treatment of older people who have had a fall can improve their wellbeing and quality of life, as well as their health. The management of the elderly patient who has fallen should begin with investigating the cause of the fall.


Thank you very much .Highly informative