When to use an Oropharyngeal (OP) airway
In an unconscious patient, the most common cause of airway obstruction is when the muscles holding the tongue relax causing the tongue to fall back into the oral cavity blocking the airway.
If it is difficult maintaining a clear airway with manual procedures alone, i.e. head tilt-chin lift or jaw thrust, then a piece of equipment known as an oropharyngeal airway may be used.
The oropharyngeal airway is a rigid, plastic device that is designed to fit over the tongue and keep it from falling to the back of the throat.
Oropharyngeal (OP) airways should only be used on unresponsive patients.
OP airways should not be used if:
- The patient is conscious
- The patient’s gag reflex is still intact
- The patient’s teeth are clenched and you have to force open their jaw
Complete obstruction of the airway will typically be silent. A snoring sound may indicate a partial blockage.
How to Insert an Oropharyngeal Airway
- Select the correct size by placing it against the patient´s face, it should extend from the centre of the lips to the angle of the jaw, alternatively, the angle of the lips to the lobe of the ear can also be used to size an OP airway. It is important to ensure the OP airway is sized correctly as an incorrectly sized OP airway can block the patient´s airway.
- Ensuring the patient´s airway is clear, insert the OP airway in a back to front position with the end of the airway facing the roof of the mouth and slide it along to the soft palate taking care not to damage the soft tissue of the mouth which may cause bleeding, adding to the airway problems.
- Rotate the OP airway 180 degrees to position it over the tongue with the flange (bite block) resting behind the lips and against the teeth.
- If the patient gags during the insertion of an OP airway it should be removed immediately as stimulating the gag reflex may induce vomiting.
- Check for correct placement by looking for chest rising and falling and
listening for air movement through the OP airway. Also, check that the lips or tongue are not caught between the flange and the teeth. - Once in place, ensure good jaw and head position to assist in keeping an open airway.
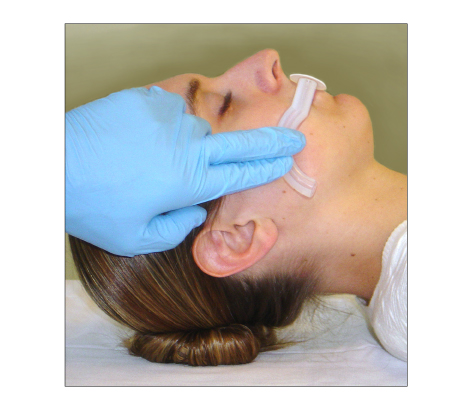
How to Size an Oropharyngeal Airway
Only remove the OP airway if the patient´s mouth becomes contaminated with fluid such as vomit, blood or saliva. If this happens, remove the airway and clear the fluid by suction or postural drainage and reinsert a fresh OP airway.
Be aware also, that as the patient recovers consciousness they will probably reject the airway by spitting or pulling it out themselves